What is an incompetent cervix?
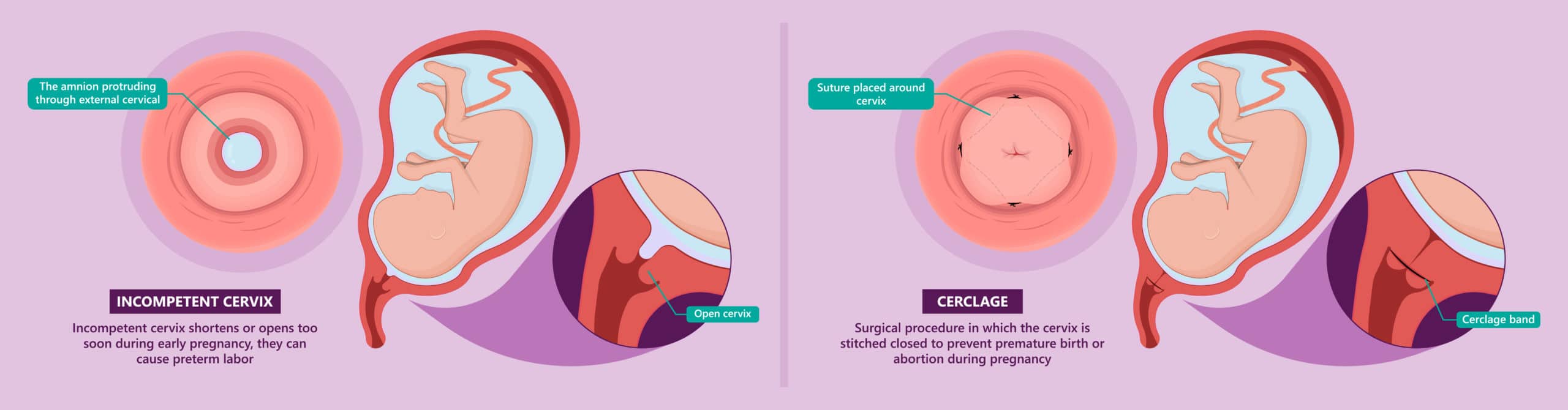
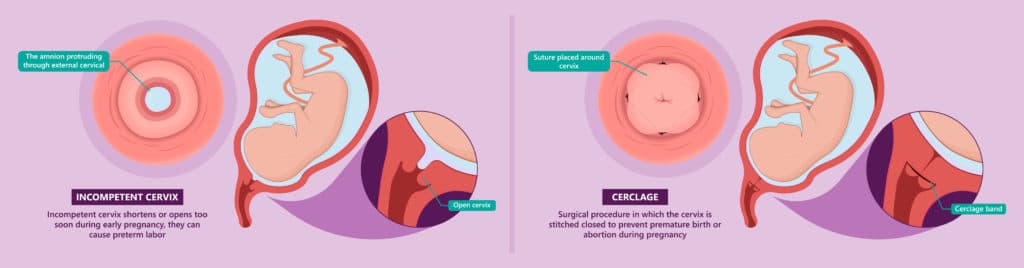
An incompetent cervix which is otherwise called Cervical insufficiency is the inability of the uterine cervix — the “gate” to the womb, to retain pregnancy, that is to hold off the fetus from being expelled, in the second trimester, leading to “unceremonious” miscarriages.
It is about the commonest cause of RECURRENT MID TRIMESTER MISCARRIAGE [ “Mid trimester” refers to the 2nd trimester; period extending from the 14th to the 26th week of gestation, that is the 4th to the 6th month of pregnancy]
Effects of incompetent cervix
Imagine being pregnant three times and still having nothing to show for it — all having been expelled unceremoniously at the mid trimester, before the age of viability, and without as much as the usual cramps that heralds miscarriages. Right.
It always follows the same sequence. You miss your period for two consecutive months. Next you pee on a stick to confirm you are preggers. Then comes the excitements and the day dreams as your tummy begins to fill out, the rush when the little nuisance inside you awakens and makes its first kick, and you begin to make the “footballer” or “karate kid” jokes….
And just when you’re about do a scan to determine the sex of the baby so you can start referring to it as a he or she, or when you are jejely going to the toilet to pee or loo, you see the head of your “little nuisance” popping out of your vagina. And before you could say Jack Robinson, it is out on the bathroom floor as a lifeless mass with WELL FORMED head, legs, hands, and even eyes and nostrils!
Your heart breaks into smithereens. Couldn’t it have happened earlier on when it was just “blood”, you know an indistinguishable mass of tissue, and save you all the stress and heart ache? It had to wait till the 5th month before happening!
They called it a “miscarriage”, but didn’t those usually come with tell-tale signs? First a warning bleed, then the severe cramps, before the expulsion of the fetus proper. But this one happened unceremoniously without much ado. And the fact that it has been recurring, three times now? Must be the work of a witch!
But, what if I told you that the woman after whom this story was fashioned just delivered a bouncing baby boy this afternoon, and that it didn’t require the kabashing of a Pastor nor the amansi [incantations] of any dibia; what if I told you that?
Take a walk with me let’s identify this “witch”, dissect it, and learn how to clip its wings.
The protective role of cervix during pregnancy
Following conception, the cervix transforms into a rigid, unyielding fortress, the main function of which is to keep the “delinquent fetus” — sentenced to 9 months imprisonment inside the womb — locked up behind bars, until after 9 months when it must have served its full sentence.
The fortress so formed leaves only a tiny tunnel, the cervical canal, for communication between the fetus and the outside. This opening is still filled in with a mucus plug to prevent any harm coming to the baby, and to keep it from using external factors to pull a Michael Scofield stunt and attempt a prison break.
To know how strong this fortress is, suffice it to say that the whole process of labour, a process that could take up to 18 hours and more, is the uterus working hard over time, trying to force the cervix open by exerting increasing pressure on it.
Cervical insufficiency thus occurs, when this fortress is INCOMPETENT and therefore unable to withstand the normal pressure mounted on it by the baby’s weight, and thus fails to keep the “delinquent fetus” behind bars, leading to the baby literary “falling off” from the womb in the 2nd trimester.
Risk Factors of cervical insufficiiency
The risk factors for cervical incompetence includes the following:
- A cervical tear during a previous delivery.
- Gynaecological procedures that involve cervical dilatation like D and C for induced abortion.
- Certain structural [congenital] anomalies of the cervix.
- Connective tissue disorders like Ehlers- Danlos syndrome.
- Exposure to DES [Diethylstilbesterol]
- Cervical cone biopsy
Clinical features; how to recognize a case of incompetent cervix
The most important finding that should raise suspicion for a possibility of cervical incompetence is a past history of an “unceremonious” mid trimester miscarriage, recurrent or not, but especially when recurrent.
Even though most of such miscarriages would be “unceremonious” — involving painless cervical dilatation, and rapid expulsion of the fetus; others may be “ceremonious”, being accompanied by subtle symptoms like mild cramps, low back pain, or heaviness in the waist, spotting and increased vaginal discharge.
Other findings that may be suggestive of cervical incompetence include:
- an ultrasound evidence of a short cervix
- funneling at the inner end of the cervix.
Secondary Prevention/Treatment of incompetent cervix
The most widely accepted treatment for an incompetent cervix, once identified, is the placement of a cerclage to reinforce the tensile strength of the cervix.
This is usually done at the beginning of the second trimester, usually between 14 and 16 weeks, and involves using of a stitch to narrow and tighten the entrance to the cervical canal, to prevent the baby from “falling off”.
Such a cerclage, when put in place, is allowed to stay insitu until after 28 weeks [usually as close to term as possible] when it is removed to allow for easy passage of the baby during delivery.
After 3 previous unsuccessful pregnancies, which all ended unceremoniously in the second trimester, the woman who inspired this story/lecture had a cerclage placed and was able to carry her pregnancy to term.
This afternoon, she was delivered of a bouncing baby boy.
And that was how we exorcised the witch responsible for her recurrent miscarriages with just a Shirodkar stitch [ thread] placed at a strategic place in her cervix.
About the author

Dr Chibuike Joseph Chukwudum is a doctor who Studied Medicine and Surgery at Nnamdi Azikiwe University Awka. He is the former Medical Officer at Oakland specialist hospital,obosi.He also previously worked at Nnamdi Azikiwe University Teaching Hospital, Nnewi, Anambra State.
-
Dr Chibuike Joseph Chukwudumhttps://medicdrive.org/author/dr-chibuike-joseph-chukwudum/
%27%20fill-opacity%3D%27.5%27%3E%3Cellipse%20fill%3D%22%232b2b2c%22%20fill-opacity%3D%22.5%22%20rx%3D%221%22%20ry%3D%221%22%20transform%3D%22matrix(-7.74894%20-26.49932%2033.2252%20-9.71573%20145.6%2022)%22%2F%3E%3Cellipse%20fill%3D%22%23f1f1f0%22%20fill-opacity%3D%22.5%22%20rx%3D%221%22%20ry%3D%221%22%20transform%3D%22rotate(-126.2%2031.3%209)%20scale(133.88831%2029.85984)%22%2F%3E%3Cpath%20fill%3D%22%236f6f70%22%20fill-opacity%3D%22.5%22%20d%3D%22M7%2057.4L42.3%20149%203.9%20163.6-31.2%2072z%22%2F%3E%3Cellipse%20fill%3D%22%237e7e7e%22%20fill-opacity%3D%22.5%22%20rx%3D%221%22%20ry%3D%221%22%20transform%3D%22matrix(26.0676%20-18.0803%2019.00828%2027.40552%20127.6%2033.7)%22%2F%3E%3C%2Fg%3E%3C%2Fsvg%3E)
-
Dr Chibuike Joseph Chukwudumhttps://medicdrive.org/author/dr-chibuike-joseph-chukwudum/

-
Dr Chibuike Joseph Chukwudumhttps://medicdrive.org/author/dr-chibuike-joseph-chukwudum/
-
Dr Chibuike Joseph Chukwudumhttps://medicdrive.org/author/dr-chibuike-joseph-chukwudum/

